The gastric bypass is a bariatric procedure that can be performed as a proximal or malabsorptive operation. The proximal Roux-en-Y gastric bypass, also known simply as gastric bypass, is a stomach restrictive operation with mild malabsorption. The malabsorptive Roux-en-Y or medial gastric bypass (MGBP) is a similar operation, but with significant malabsorption.
During a robot-assisted gastric bypass procedure, a small stomach pouch is created, restricting the amount of food that can be consumed. In addition, the top one-fourth of the small intestine is bypassed. Weight loss is achieved through both restriction of food consumption and a mild decrease in calorie absorption.
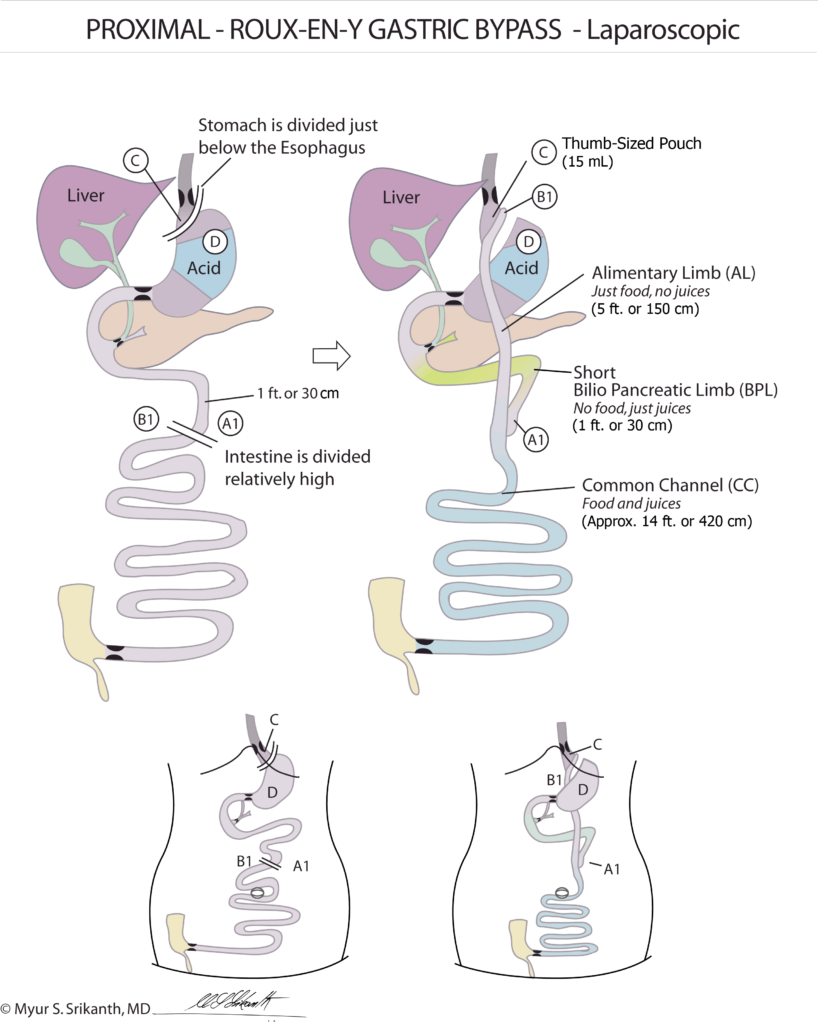
The stomach is divided vertically to create a small, thumb-sized pouch (approximately 15 ml). Patients usually report feeling full after eating about 2 ounces of solid food. The upper small intestine is divided and the lower section is attached directly to the small stomach pouch. The food travels through this portion of the small intestine (alimentary limb or AL) until it meets with the section of intestine carrying digestive (bile and pancreatic) juices, which is called the bilio-pancreatic limb (BPL). The last segment of the intestine where the food and digestive juices mix is referred to as the common channel (CC). Absorption of nutrients and calories is determined by the length of the common channel, and a short common channel decreases the risk for weight regain by decreasing calorie absorption.
Proximal Gastric Bypass Outcomes
Weight Loss
Approximately 60 to 70 percent excess weight loss has been reported.1
Improvement / Resolution of Comorbidities
Improvement/resolution in all major comorbidities has been documented, including type 2 diabetes, sleep apnea, hypertension, high cholesterol and GERD.
How Malabsorptive (Medial) Gastric Bypass (MGBP) Works
This medical gastric bypass variation is a stomach-restrictive operation with significant malabsorption. A small stomach pouch is created, very similar to the one created with the proximal gastric bypass. This operation differs from the proximal gastric bypass in that roughly two-thirds to three-fourths of the small intestine length is bypassed, resulting in a significant decrease in calorie absorption. Weight loss is achieved both through restriction of food consumption and malabsorption.
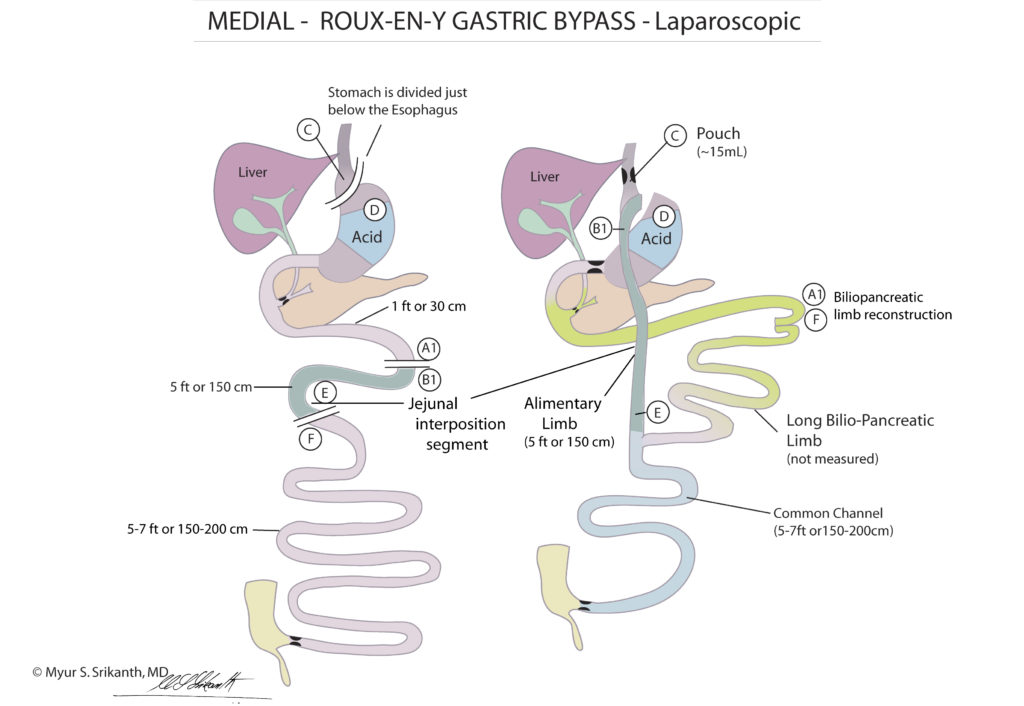
The stomach is divided vertically to create a small, thumb-sized pouch (approximately 15 ml). Patients usually report feeling full after eating about 2 ounces of solid food. The mid small intestine is divided and the lower section is attached directly to the small stomach pouch. The food you consume travels through this portion of the small intestine until it meets with the top portion of intestine that carries digestive juices (bile and pancreatic juices). This section, referred to as the bilio-pancreatic limb or BPL, is much longer than in the proximal gastric bypass and is connected 60 – 80 inches (5 – 7 feet) from the large intestine (colon). This last one-third to three-fourths of the total small intestinal length where the food stream and intestinal juices mix together is where absorption occurs and is called the common channel (CC). Absorption of nutrients and calories is determined by the common channel length, so a short common channel decreases the risk for regaining weight by decreasing calorie absorption from fats and complex carbohydrates.
Malabsorptive Roux-en-Y Gastric Bypass Outcomes
Weight Loss
About 80 percent excess weight loss (EWL) has been reported.2
Improvement / Resolution of Comorbidities
Improvement/resolution in all major comorbidities has been documented, including type 2 diabetes, sleep apnea, hypertension, high cholesterol and GERD.
Effective Weight Loss
Weight loss is achieved through stomach restriction as well as malabsorption, making this surgery a better option for patients with a high BMI and for those who fail to achieve adequate weight loss after the proximal gastric bypass. This operation typically provides predictable weight loss with good long-term weight loss maintained.