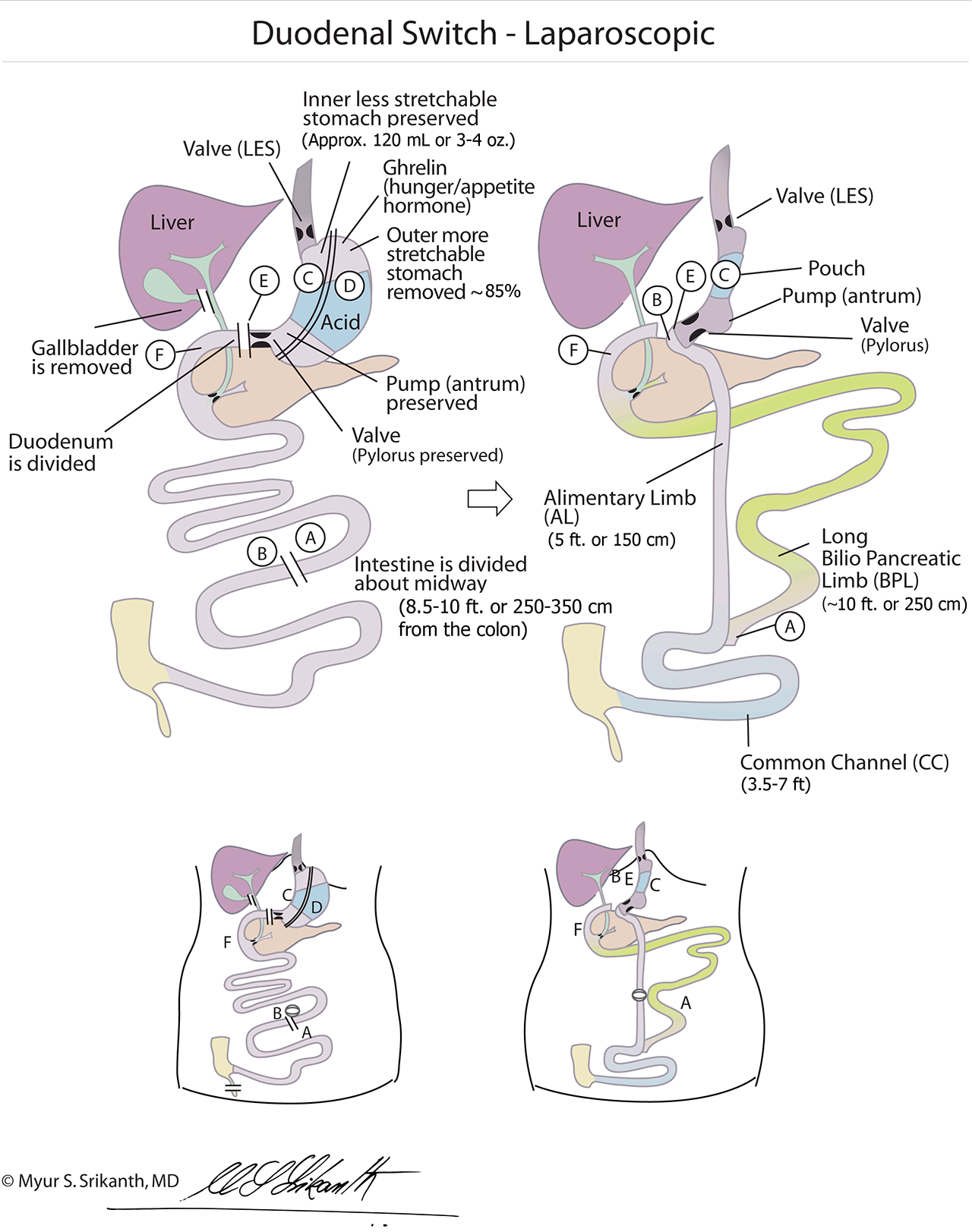
The duodenal switch (DS) surgery enables patients to eat a normal meal in much smaller quantities. This operation restricts food consumption by removing the most stretchable portion of the stomach, similar to a sleeve gastrectomy. Additionally, calorie absorption is limited by bypassing roughly one-half to three-fourths of the upper small intestine.
A sleeve gastrectomy is performed to remove the stretchy upper and outer 85 percent of the stomach, leaving a small, vertically-oriented tubular stomach. Stomach capacity is reduced from about a quart (1,000 ml) to roughly 4 – 6 ounces (120 – 180 ml). Depending on the size of the tube (bougie) that is created, patients generally report feeling full after eating 4 – 6 ounces of solid food.
The important structural elements of the stomach — such as the antrum, the pylorus and the nerves that control stomach function — are preserved. The result is a much smaller stomach that functions similarly to a normal one. This allows patients to enjoy a relatively normal diet (albeit in much smaller quantities) without side effects such as “dumping” syndrome.
A duodenal switch (DS) weight loss surgery involves rerouting some small intestine to reduce calorie absorption. The duodenum (the first section of the small intestine) is divided and connected to the last 7 – 13 feet (225 – 400 cm) of small intestine through which the food passes (alimentary limb or AL). The top half of the intestine carries only digestive (bile and pancreatic) juices and is called the biblio-pancreatic limb (BPL). This section is reconnected to the food stream 3.5 – 10 feet (100 – 300 cm) from the colon (large intestine). The last segment of the intestine —where the food and digestive juices mix — is referred to as the common channel (CC). Absorption of nutrients and calories from complex carbohydrates and fats is determined by the length of the CC. Absorption of calories from simple carbohydrates, such as starches, occurs in the alimentary limb. The shorter the AL the more the weight loss. The longer the CC the lesser the risk for nutritional problems.
The removal of the upper and outer stretchable portion of the stomach results in a decrease in the level of ghrelin, the “hunger hormone,” which reduces the appetite. In addition, bypassing the upper intestine helps bring food to the lowest portion of the small intestine earlier than usual, releasing important appetite-suppressing hormones such as GLP1 and polypeptide YY (PYY). This accounts for the superior weight loss, weight maintenance and diabetes resolution associated with this surgery.
LAP DUODENAL SWITCH OUTCOMES
Weight Loss
Approximately 75 to 80 percent excess weight loss has been reported.1,2 This procedure typically is recommended for patients who suffer from clinically severe obesity or are at a high risk for obesity-related diseases, including Type 2 diabetes, metabolic syndrome, elevated lipids i.e., hyperlipidemia, hypercholesterolemia, hyperlipidemia and hypertension. Compared to gastric bypass and other forms of bariatric surgery, the amount of weight lost with duodenal switch can be significantly higher.
Improvement / Resolution of Comorbidities
Improvement or resolution of all major comorbidities has been documented, including type 2 diabetes, sleep apnea, hypertension and high cholesterol. A very high cure rate for diabetes has been reported with this surgery. 3,4
Advantages
The risk of “dumping” syndrome is very low. The symptoms of dumping syndrome are nausea, cramping, diarrhea, sweating, vomiting and heart palpitations, and it can occur when a patient (who has had gastric bypass) consumes sugar or carbohydrates, or eats too quickly.
Medication Tolerance
The duodenal switch sleeve procedure is pill-friendly, allowing patients to better tolerate medications including aspirin and other NSAIDS.
Suited For
The duodenal switch bariatric surgery is a good option for all patients with severe obesity BMI (35 or greater), diabetes or metabolic syndrome. 5,6,7,8,9 Typically, these patients have already tried diet and exercise to lose weight, but without much success. Additionally, a good candidate would be someone who has been through a weight loss procedure and is now looking for a Revision from a Sleeve Gastrectomy to a Duodenal Switch.
TRUST CENTER FOR WEIGHT LOSS SURGERY
As Seattle’s leading weight loss surgery center, Center for Weight Loss Surgery is home to numerous expert surgeons, so you can be confident that you’re receiving exceptional, personalized care. Reach out anytime to ask questions about or book a consultation for a Duodenal Switch in Seattle. Click here to read success stories from some of our patients.
After a duodenal switch procedure, what is the weight loss timeline? According to the latest research, patients who undergo this surgery experience the vast majority of their weight loss within the first one to two years. In many cases, patients are able to maintain the weight loss for at least five years. Although each patient’s specific circumstances are different, these are the most typical results.
Is duodenal switch painful? Patients are likely to experience some swelling and pain in the area of the incision, which is normal. These improve over time as the body heals. Depending on the patient, there also may be occasional bloating, acid reflux and/or intestinal irritation after recovery. It is recommended that patients talk to their doctors about all the potential complications when considering this procedure.
How long does a duodenal switch surgery take? The procedure itself takes about three to four hours in most circumstances. Afterwards, patients can expect a recovery period of about three to four weeks.
Can you drink coffee after a duodenal switch? Surgeons typically recommend patients restrict their coffee consumption after this surgery. This is because the caffeine can induce dehydration, gastric reflux and hinder the body’s ability to absorb certain nutrients.
References
Strain GW, et al. Comparison of effects of gastric bypass and biliopancreatic diversion with duodenal switch on weight loss and body composition 1–2 years after surgery. Surgery for Obesity and Related Diseases. 2007;3(1):31–36.
Nelson DW, Blair KS, Martin MJ. Analysis of Obesity-Related Outcomes and Bariatric Failure Rates with the Duodenal Switch vs Gastric Bypass for Morbid Obesity. Arch Surg. 2012;147(9):847–854. doi:10.1001/archsurg.2012.1654.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric Surgery: A Systematic Review and Meta-analysis. JAMA. 2004;292(14):1724–1737. doi:10.1001/jama.292.14.1724.
Hedberg J1, Sundbom M. Superior weight loss and lower HbA1c 3 years after duodenal switch compared with Roux-en-Y gastric bypass--a randomized controlled trial. Surg Obes Relat Dis. 2012 May-Jun;8(3):338-43. doi: 10.1016/j.soard.2012.01.014. Epub 2012 Feb 1.
Hilde Risstad, MD1,2; Torgeir T. Søvik, MD, PhD3; My Engström, RN, PhD4; et al. Five-Year Outcomes After Laparoscopic Gastric Bypass and Laparoscopic Duodenal Switch in Patients With Body Mass Index of 50 to 60A Randomized Clinical Trial. JAMA Surg 2015;150(4):352-361
Skogar ML1, Sundbom M2. Duodenal Switch Is Superior to Gastric Bypass in Patients with Super Obesity when Evaluated with the Bariatric Analysis and Reporting Outcome System (BAROS). Obes Surg. 2017 Sep;27(9):2308-2316. doi: 10.1007/s11695-017-2680-z.
Topart P1, Becouarn G, Ritz P. Weight loss is more sustained after biliopancreatic diversion with duodenal switch than Roux-en-Y gastric bypass in superobese patients. Surg Obes Relat Dis. 2013 Jul-Aug;9(4):526-30. doi: 10.1016/j.soard.2012.02.006. Epub 2012 Mar 3.