Stomach Intestinal Pylorus Sparing (SIPS) Weight Loss Surgery
The single anastomosis duodenal-ileal bypass is a novel approach to weight loss surgery. It is also referred to as the stomach intestinal pylorus sparing (SIPS) surgery, loop duodenal switch (DS) surgery or single anastomosis duodenal switch surgery.
Weight loss is induced by restricting the quantity of food consumed and the amount of calories absorbed, which results in good weight loss and maintenance of this weight loss.
The SADI-S/SIPS procedure brings about weight loss in a few different ways, namely:
Surgical Restriction for Reduced Stomach Capacity
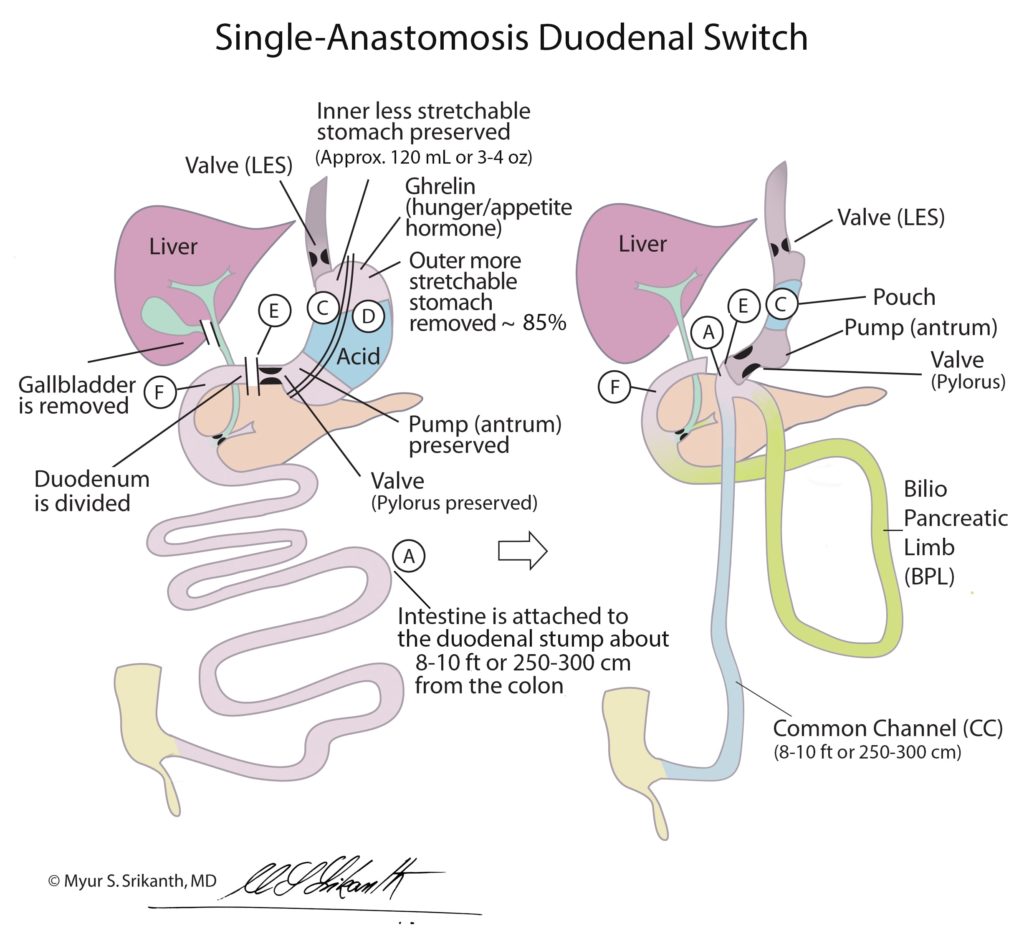
Restriction of food consumption is achieved with a vertical sleeve gastrectomy surgery, where a small stomach tube is created by removing the outer 85-90% of the stretchable portion, which reduces stomach capacity from about a quart (four cups or 32 ounces) to roughly half a cup (four to six ounces).
The key structural elements of the stomach are preserved, such as the:
Pyloric valve: The pyloric valve regulates when and how much food leaves the stomach tube to allow enough time to churn it down to the appropriate consistency.
Vagus nerve: This nerve controls the pyloric valve.
Antrum: The antrum is the pump that pushes food across the pylorus into the beginning of the small intestine (also referred to as the duodenum).
The procedure leaves a much smaller stomach that functions normally. With the SADI-S / SIPS procedure, patients can eat a relatively normal diet and feel satisfied with smaller quantities.
Malabsorption
In a loop duodenal switch surgery, the upper half of the small intestine is bypassed, moderately reducing calorie absorption. The first section of the small intestine, called the duodenum, is divided just beyond the pyloric valve, re-directing the food into the bottom half of the small intestine. The bypassed upper small intestine is called the biliopancreatic limb (BPL) because it only carries the bile and pancreatic juices.
The segment of the small intestine between the duodenum and colon through which the food travels is called the alimentary limb (AL). Since this segment is a common pathway for food and digestive juices, it is also referred to as the common channel (CC). Nutrient and calorie absorption is determined by the length of the AL/ CC. A shorter AL/CC decreases calorie absorption, minimizing weight regain risk.
Gastrointestinal (GI) Hormonal Changes
Removing the stomach’s upper and outer stretchable portion decreases ghrelin levels, reducing hunger and appetite. Rerouting the intestine means food arrives at the small intestine’s lowest portion sooner than usual, releasing hormones, such as GLP-1 and PYY, that help suppress appetite by slowing gastric emptying and inducing satiety, stimulating pancreatic insulin secretion and suppressing pancreatic glucagon levels. Through these GI hormonal changes, SADI surgery induces significant weight loss, better weight maintenance and diabetes remission.
As with sleeve gastrectomy surgery, the stretchy upper and outer 85 percent of the stomach is removed leaving a small, tube-shaped stomach. Stomach capacity is reduced from about a quart (1,000 ml) to roughly 4 – 6 ounces (120 – 180 ml). Depending on the size of the tube (bougie) that is created, patients generally report feeling full after eating 4 – 6 ounces of solid food.
Reasons to Consider the Single Anastomosis Duodenal Switch
SADI is similar to the traditional duodenal switch surgery. The main difference is that in SADI bariatric surgery, the small intestine is divided at one point rather than two.
SADI is a suitable option for those who have tried to lose weight through diet and exercise without seeing desirable results. It may also be ideal for individuals who are looking for ways to maintain long-term weight loss and those seeking better control of diabetes. In patients who have had a previous vertical sleeve gastrectomy and are looking to improve their weight loss outcome, we could add SADI as a Sleeve Enhancement Procedure.
Advantages
Predictable weight loss: Because weight loss occurs through stomach restriction and malabsorption, individuals can experience predictable weight loss with good weight maintenance. Patients experience similar weight loss to the DS with potentially fewer malabsorptive symptoms.
No risk of dumping syndrome: Food is held within the sleeve gastrectomy by the pylorus, which only allows a small amount of it into the intestine, minimizing the risk of dumping syndrome.
Weight loss: Approximately 75 percent excess weight loss has been reported.1
Medication tolerance: After a pill-friendly SIPS weight loss procedure, aspirin and other NSAIDs are well tolerated.
Improvement / Resolution of Comorbidities
Patients have experienced improvement or resolution of all major comorbidities, including type 2 diabetes, sleep apnea, hypertension and high cholesterol. 2
Contact Our Seattle Team to Learn More About SADI-S or SIPS Weight Loss Surgery
With clinics in Kirkland and Federal Way, WA, the Center for Weight Loss Surgery is Seattle’s premier bariatric center, dedicated to helping you revitalize your life and achieve your healthy living goals.
We realize that every individual has unique needs, which is why we offer personalized care throughout the surgery experience. Our team will conduct a comprehensive assessment to determine the best option for you. Most of the process can be completed virtually to accommodate traveling patients.
Schedule a consultation today to learn if the SADI-S or SIPS weight loss surgery is the best option for you.
References
Sánchez-Pernaute A, et al. Single-anastomosis duodenoileal bypass with sleeve gastrectomy: metabolic improvement and weight loss in first 100 patients. Surgery for Obesity and Related Diseases. 2013;9(5):731–735.
Lee W-J, et al. Duodenal–jejunal bypass with sleeve gastrectomy versus the sleeve gastrectomy procedure alone: the role of duodenal exclusion. Surgery for Obesity and Related Diseases. 2015;11(4):765–770.